
by Ayaka J. Iwata, MD; Ralph P. Tufano, MBA, MD; Elizabeth N. Pearce, MD; and Gregory W. Randolph, MD
Voice changes are important considerations in thyroid surgery. Thyroidectomy, the removal of part or the whole thyroid gland, is a commonly performed operation that is done for myriad reasons, including thyroid cancers, nodules, goiter (thyroid enlargement), and hyperthyroidism (overactive thyroid). Sometimes the disease process itself can affect the voice, but thyroid surgery too can cause voice disturbances that musicians, especially singers, should be aware of.
Thyroid Function and Anatomy
The thyroid is a butterfly-shaped gland that sits in the lower front of the neck. It has a right lobe and a left lobe that are connected by the isthmus, or a bridge of thyroid tissue. It secretes hormones that control our overall metabolism, growth, and development. The amount of thyroid hormone produced by the gland is controlled by another hormone called the thyroid stimulating hormone (TSH), which is produced by the pituitary gland.
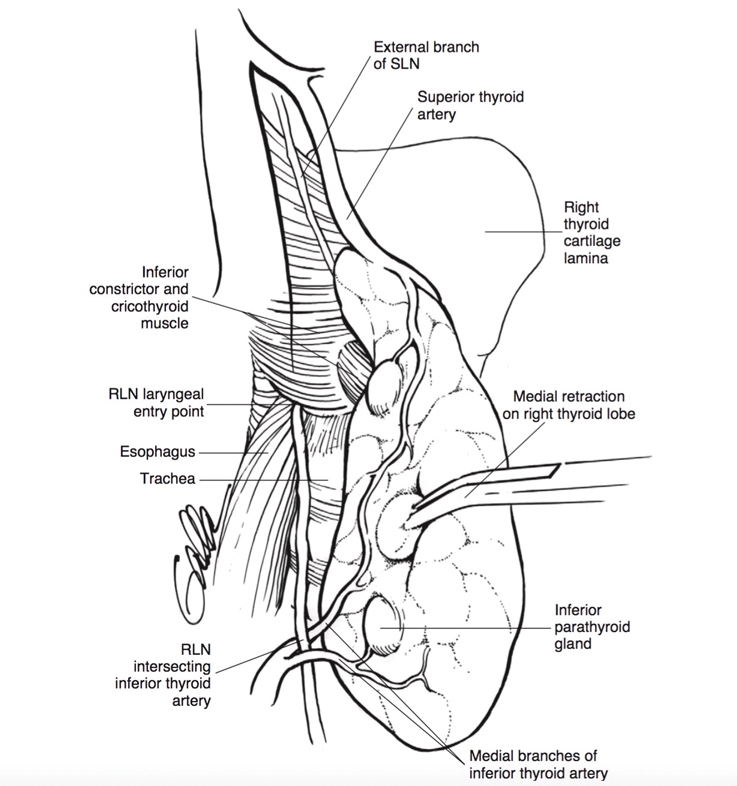
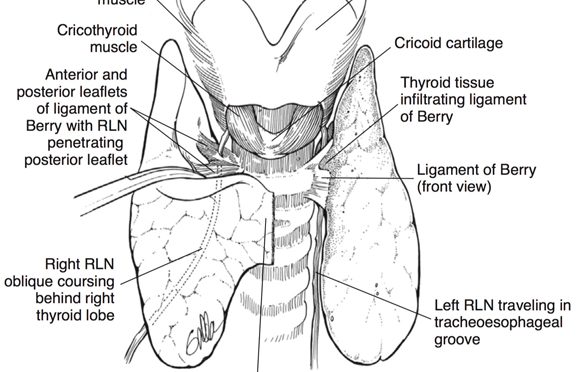
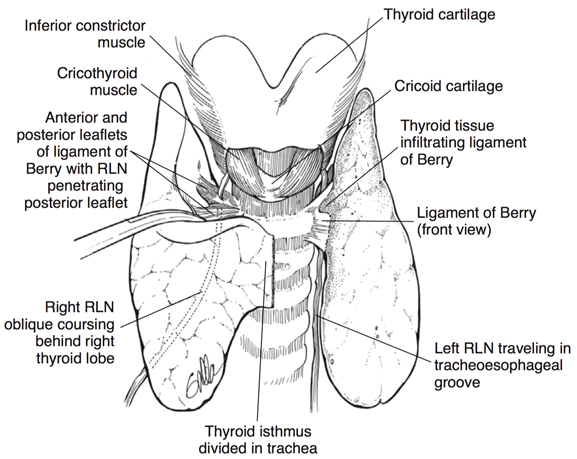
Located close to the thyroid gland are two nerves on each side of the neck that control the human voice. The major one is called the recurrent laryngeal nerve (RLN), which travels right behind the thyroid gland. It controls all but one of the muscles that open and close the vocal cords, and are important for the voice, and for breathing and swallowing. The second nerve is the superior laryngeal nerve (SLN). The internal SLN branch provides sensory information from the top part of the voice box and the external branch controls the cricothyroid muscle. This muscle helps project the voice and create higher pitch registers.
Thyroid Nodules
Thyroid nodules are abnormal growths of thyroid cells that form lumps within the gland. They most commonly do not produce any symptoms. They are usually discovered during an examination by a healthcare provider, or incidentally during imaging studies ordered for unrelated reasons.
Nodules are very common, with more than half of us possessing thyroid nodules by the time we reach our 60s. Luckily, the vast majority of thyroid nodules are benign (non-cancerous). However, as 7 to 15% of nodules harbor thyroid cancer, it’s important not to disregard them.
The typical clinical workup starts with a thyroid ultrasound, which reveals the size, shape, and features of the nodule. Depending on these findings, the physician may recommend a biopsy, called a fine needle aspiration. Based on these results, the physician may recommend surgery.
How the Voice Can Be Affected
On rare occasions, the voice can be affected by an aggressive thyroid cancer that directly invades the RLN, making the vocal cord weak or paralyzed. As a result, the patient may already have voice changes by the time they see the thyroid surgeon. The voice can still be normal, however, if the other normal vocal cord compensates well. For this reason, many patients undergoing thyroid surgery should undergo a preoperative assessment of their larynx (voice box) through a laryngoscopy. This is an in-office procedure where a thin flexible scope is guided through the nose and throat to directly view the vocal cords. Finding a paralyzed or weakened vocal cord in the setting of a thyroid nodule implies cancer and is important in planning the extent of surgery and discussing further treatment.
Temporary or permanent damage to the voice can also be a result of the surgery itself. This may occur in some form in as much as 10% of patients undergoing surgery, although it is less common with experienced thyroid surgeons. Since the RLN is close to the thyroid gland, it can be injured during surgery. Such RLN injury can result in hoarseness, a breathy voice, or vocal fatigue. Laryngoscopy after surgery in such a case will reveal a weak or immobile vocal cord. In these cases, musicians who blow into their instruments, such as brass and woodwind players, may initially notice some difficulty taking in a full breath.
A less common surgical cause of voice change is SLN injury. This can manifest as voice fatigue, inability to project the voice, or difficulty in pitch modulation. Post-operative laryngoscopy findings here are often subtle and may be seen as normal—SLN injury, therefore, is difficult to diagnose. Other causes of voice disturbance after surgery include irritation or swelling of the vocal cords from the breathing tube necessary for general anesthesia, injury to the muscles in the neck during the dissection, or scarring.
Intraoperative Nerve Monitoring
The majority of surgeons in the US now commonly employ intraoperative nerve monitoring (IONM) during thyroid surgeries, which may be used to help with nerve identification and confirm nerve function. It is especially useful in high-risk surgeries, such as in advanced thyroid cancer, complex surgery, or reoperations. It is also important during total thyroidectomies (removing the entire thyroid gland) as it allows surgeons to test the integrity of the nerve after they complete one side of the thyroidectomy before committing to moving on to the opposite side. This helps avoid inadvertently injuring both RLNs, which can result in severe airway compromise. Finally, as the EBSLN is not always visible during dissection, IONM allows for a consistent way to monitor the integrity of this nerve, which is critical for the professional singer.
Rehabilitation After Surgery for Singers
Nerve damage after surgery may improve over the course of a few months, but may also never fully recover. Several treatment options exist, and should be discussed. Voice physical therapy can be useful, as can vocal cord surgeries in some cases. Professional singers are like fine-tuned athletes, and may find re-training through vocal rehabilitation helpful during recovery even for uncomplicated surgery. A professional coach or a speech language pathologist can help guide patients through this process. Successful therapy can not only improve a patient’s professional performance, but their quality of life as well, and is a crucial part of the healing process.
Luckily, thyroid disease or surgery generally do not affect the professional life of musicians who do not use their vocal cords. Violinists or violists who place their instruments against their necks may note some changes in the sensitivity of their skin due to the scar after surgery. This is usually temporary, and typically does not affect a musician’s ability to play.
Disclaimer: Please make sure you consult with your personal physician before making any personal medical decisions or undertaking any medical procedures.